
Treatment options vary, depending on the type of cancer and how far it has grown and spread. See the separate leaflets on the specific cancers for more details. There is also another leaflet called Cancer – Staging and Grading Cancer’ which discuses how a cancer is classified depending on its type (grading) and how far it has spread in the body (staging). Briefly, the three most common treatments are:
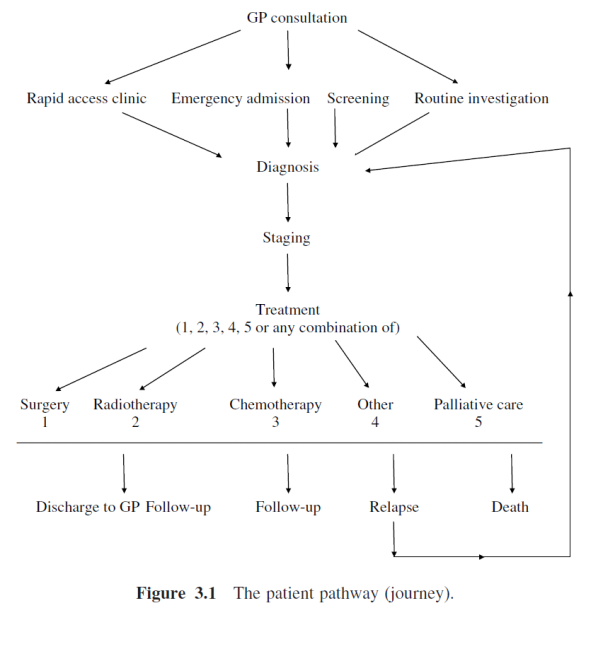
Treatment Options
It may be possible to cut out a malignant tumour.
This is a treatment that uses anticancer drugs to kill cancer cells, or to stop them from multiplying: There are various different types of drugs used for chemotherapy. The drug or combination of drugs selected depends on the type of cancer being treated.
This is a treatment that uses high-energy beams of radiation which are focused on cancerous tissue. This kills cancer cells, or stops cancer cells from multiplying.
High-dose chemotherapy may damage bone marrow cells and lead to blood problems. However, if you receive healthy bone marrow after the chemotherapy then this helps to overcome this problem.
This is where drugs are used to block the effects of hormones. This treatment may be used for cancers that are hormone-sensitive such as some cancers of the breast, prostate and uterus (womb).
Some treatments can boost the immune system to help to fight cancer. More specific immunotherapy involves injections of antibodies which aim to attack and destroy certain types of cancer cells. Research is underway to try to find vaccines that would stimulate your own immune system to make antibodies against cancer cells.
This is a new area of possible treatments. Research is underway to find ways of blocking, repairing or replacing abnormal genes in cancer cells.
These can sometimes be used to cut off the blood supply to tumours. The tumour then dies.
Scientists’ understanding of the biology of cancer cells has led to the development of biological agents that mimic some of the natural signals that the body uses to regulate growth. This cancer treatment, called biological response modifier (BRM) therapy, biologic therapy, biotherapy, or immunotherapy, has proven effective for several cancers through the clinical trail process. Some of these biologic agents, occurring naturally in the body, can now be produced in the laboratory. Examples are interferons, interleukins, and other cytokines. These agents are given to patients to imitate or influence the natural immune response agents either directly altering the cancer cell growth or acting indirectly to help health cells control the cancer. One of the most exciting applications of biologic therapy has come from identification of certain tumour targets, called “antigens”, and aiming an antibody at these targets. This was first used as a means of localizing tumours in the body for diagnosis and more recently has been used to attack cancer cells.
For some cancers, a combination of two or more treatments may be used. A range of other treatments may also be used to ease cancer-related symptoms such as pain.
For cancers that need hormones to grow, hormonal therapy can be an option. With this therapy, the production of hormones is reduced through surgery or medication. Complementary or alternative therapy Complementary and alternative therapies are treatments that do not use known cancer drugs, or use approaches not common in the medical community. Some (such as relaxation, visualization, and acupuncture) are so commonly used to control symptoms, that they are really mainstream approaches. It is important to research and understand the risks and benefits of these therapies. The National Centre for Complementary and Alternative Medicine (NCCAM) Clearinghouse (listed with the resources at the end of this section) is a good source of information.
Until the late 1990s nearly all drugs used in cancer treatment (with the exception of hormone treatments) worked by killing cells that were in the process of replicating their DNA and dividing to form 2 new cells. These chemotherapy drugs also killed some normal cells but had a greater effect on cancer cells. Targeted therapies work by influencing the processes that control growth, division, and spread of cancer cells, as well as the signals that cause cancer cells to die naturally (the way normal cells do when they are damaged or old). Targeted therapies work in several ways.
a. Antisense oligodeoxynucleotides and small interfering RNA (siRNA). An example of this is a new class of targeted therapies called PARP inhibitors. (PARP is short for poly (ADP-ribose) polymerase enzymes.) Cancer cells use PARP to repair DNA damage, including the damage caused by cancer treatment. Recent studies in breast cancer have shown that blocking PARP can make cancer cells more sensitive to treatment and promote cell death. BRAF is another gene that can produce a mutant cancer protein seen in about half of all melanomas. The drug vemurafenib (Zelboraf) targets this mutation. This drug prolonged overall survival in patients with inoperable melanoma compared to the standard drug dacarbazine. Vemurafenib was FDA approved in August 2011 for patients who have melanoma with this gene mutation.
b. Growth signal inhibitors During the 1980s, scientists found that many of the growth factors and other substances responsible for recognizing and responding to growth factor are actually products of oncogenes. Among the earliest targeted therapies that block growth signals are trastuzumab (Herceptin), gefitinib (Iressa), imatinib (Gleevec), and cetuximab (Erbitux). Current research has shown great promise for these treatments in some of the more deadly and hard-to-treat forms of cancer, such as non-small cell lung cancer, advanced kidney cancer, and glioblastoma. And second-generation targeted therapies, like dasatinib (Sprycel) and nilotinib (Tasigna), have already been found to produce faster and stronger responses in certain types of cancer and were better tolerated.
c. Angiogenesis inhibitors. Anti-angiogenesis agents are types of targeted therapy that use drugs or other substances to stop tumours from making the new blood vessels they need to keep growing. This concept was first proposed by Judah Folkman in the early 1970s, but it wasn’t until 2004 that the first angiogenesis inhibitor, bevacizumab (Avastin), was approved. Currently used to treat advanced colorectal, kidney, and lung cancers, bevacizumab is being studied as treatment for many other types of cancer, too. And many new drugs that block angiogenesis have become available since 2004.
d. Apoptosis-inducing drugs Apoptosis is a natural process through which cells with DNA too damaged to repair – such as cancer cells – can be forced to die. Many anti-cancer treatments (including radiation and chemo) cause cell changes that eventually lead to apoptosis. But targeted drugs in this group are different, because they are aimed specifically at the cell substances that control cell survival and death.
e. Nanotechnology: New technology for producing materials that form extremely tiny particles is leading to very promising imaging tests that can more accurately show the location of tumours. It also is aiding the development of new ways to deliver drugs more specifically and effectively tocancer cells
This term refers to manipulation of surgical instruments remotely by robot arms and other devices controlled by a surgeon. Robotic systems have been used for several types of cancer surgery; radical prostatectomy is among the most common uses in surgical oncology. As mechanical and computer technology improve, some researchers expect future systems will be able to remove tumours more completely and with less surgical trauma.
Copyright ©2018 all rights reserved
Designed by Purpleno.in